


Autonomous medicine, diabetes, and collapse
by Bathtub Insulin Enthusiast
Editor’s note: This piece appeared in the 2025 Almanac, however the footnotes and citations were left out due to an editorial error. The full intended piece goes below.
Those of us who seek realistic, immediate responses to ongoing collapse often receive a variety of questions that can be boiled down to “How could we ever, possibly, survive outside of capitalism, ecological extraction, or global trade?”
In some spaces, a classic variant of this line of questioning is: “What about the diabetics?” Usually, I’ve seen this question asked hypothetically and in bad faith, detached from the very much ongoing insulin crisis—a “gotcha” to shut down the possibility of ever living differently and nothing more. When the question is asked in self interest, or curiosity, well-meaning folks sometimes respond with gestures to autonomous work, mutual aid, and so on; but they rarely offer concrete application of these principles. This rhetorical back-and-forth tokenizes disabled people and accomplishes nothing of value.
I am a prediabetic, off-grid herbalist dropout collaborating with diabetic friends, and I would like to show you what this question means to our lives.
Industrial Western Medicine (IWM) does not imagine a world without itself, and so there are not high-quality evidence-based approaches to navigating diabetes in collapse available in the established scientific literature. When we embark on autonomous medical treatment, we necessarily assume the role of self-researchers: utilizing tradition, anecdote, low-quality scientific evidence, and experimentation. This is a process with pros and cons, but one that we may use together for mutual benefit when we reject hierarchical patient-provider relationships.
Claims marked with *asterisks are either anecdotal or drawn from synthesis too diffuse to enumerate here.
Diabetes mellitus is best understood as a group of several related diseases involving high blood sugar caused by some sort of disruption with how the hormone insulin is produced or utilized. Insulin binds to insulin receptors in our cells, allowing the cells to accept sugar from the blood and turn it into energy–like a key opening a lock. A long story very short, sugar that stays in the blood is not getting into our cells to power our bodies. If no sugar makes it into our cells, we will die. Secondary complications arise as sugar in the blood makes the blood thicker. This stresses the heart muscle and vein membranes, causing cardiovascular problems and issues like slow wound healing. These secondary complications can also be fatal.It is currently unknown by western science what causes diabetes; though a few vectors increase risk, such as genetics, 2nd generation antipsychotic medication,1 poor diet, and alcohol use. While body weight is often discussed around diabetes, correlation between high weight and diabetes is not as high as some imply and causative relationships are not proven.2,3
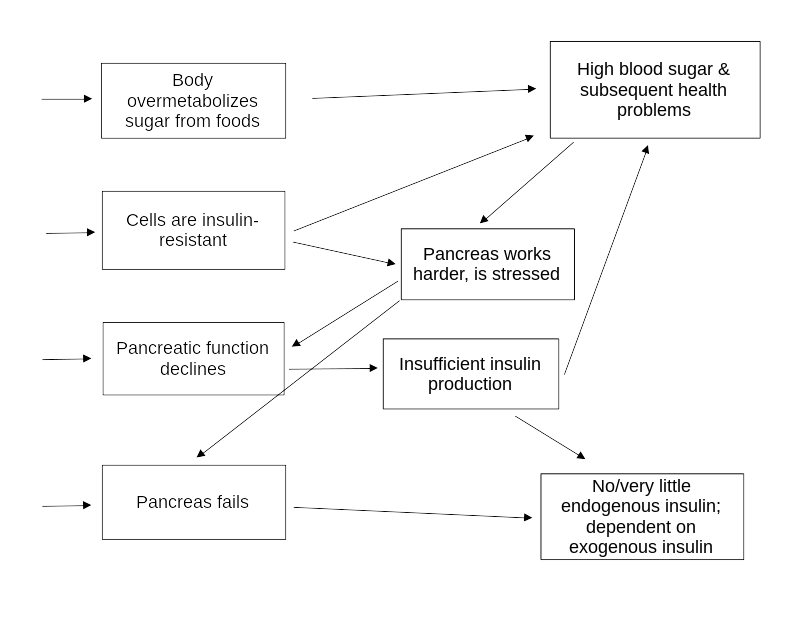
For this piece it is most important to understand that some cases of diabetes begin with or necessitate dependence on injected (exogenous) insulin;4 whereas other cases of diabetes, or prediabetes, can be managed without exogenous insulin but will progress to insulin dependence along variable but known paths if untreated (see graphic).
IWM treats diabetes in three main ways:
- Therapeutic diet
- Hypoglycemic medications, such as metformin5
- Exogenous insulin
While IWM broadly tries to prevent prediabetes and non-insulin-dependent diabetes from becoming insulin-dependent, it still assumes exogenous insulin will be available should patients require it in the future. We do not have that luxury.
Insulin must be refrigerated. It is harder for homeless and broke off-grid people to keep insulin than it is to get it. State and NGO medical access programs are location-based and expect patients to remain within a small geographical area: this can be life-threatening, as we understand the homelessness crisis increasingly as a climate refugee crisis. Thus, we have two viable treatment options: therapeutic diet, and herbs with hypoglycemic or otherwise supportive actions.
To be workable, the strategies currently available to us still require a sufficient amount of endogenous insulin—meaning they are not feasible as complete treatment for insulin-dependent diabetics. Some biohacking groups seek to produce insulin at a localized community scale.6,7 However, many of the current active projects have the vulnerability of reliance on access to industrially-produced organic solvents and machined lab equipment. Insulin from animal sources, such as the bovine and pig insulin used for much of the 20th century, may be a more feasible route in scenarios of fast-paced industrial collapse.8
Food- and herb-based treatment strategies are immediately available, though continued autonomous research is necessary. Early intervention in diabetes and prediabetes can prevent insulin dependence,9 and these strategies can support safer insulin rationing in scarcity or acute crisis.* Holistic intervention may be able to mitigate secondary complications, buying time for other solutions and improving quality of life.
The goal of a therapeutic diet for diabetes is to limit blood sugar spikes and thus demand on the pancreas. Limiting simple carbohydrates, which are metabolized most quickly into glucose, is a keystone. Proteins have very limited impact on blood glucose levels,10 but very high protein diets seem adequate for maintaining energy.* Combining carbohydrates with oils (unsaturated fats) can blunt glycemic response.11 Saturated fats can increase insulin requirements and spike blood sugar, though this could vary by individual.12 IWM-prescribed therapeutic diets sometimes make no distinction between lean/light and fatty/dark meats,* but some people have strong glycemic responses to pork, beef, and duck.*
Maintaining a therapeutic diet can be prohibitively expensive, although it is somewhat easier in warmer seasons with significant foraging. Many people who attempt therapeutic diets struggle to maintain adequate nourishment,* thus risking weight loss/weight cycling related health problems.13 Snack foods and foods that are easy to prepare are particularly difficult: communal support in procuring and preparing food is extremely meaningful in making therapeutic diets successful.
The table below shows forageable and cultivated foods we have appreciated, which we encourage farmers and food foresters to consider as a means of extending solidarity. All foods were selected for nutrient & caloric density taking into account production/procurement effort and yield in addition to stated reasons.
| Foods | Reason | Foods | Reason |
| Hearty greens (dandelion, dock, collards, turnips, nettles, etc.) | High fiber; can be used to bulk out meals instead of starches | Legumes (domesticated beans, mouse beans, peanuts) | High in protein, unsaturated fats. |
| Tree nuts (walnuts, chestnuts, hazelnuts, hickory, acorns) | High in protein, unsaturated fats. Good snacks! | Eggs (duck & chicken) | High in protein, unsaturated fats; low saturated fats |
| Fish (catfish, crawdads) | Unsaturated fats | Lean meats (rabbit, some fowl) | High in protein, lower in saturated fats |
| Sweet potatoes | Higher protein/lower carb than white potatoes | Sunflowers | Source of unsaturated fats (as oil, nut meal, snacks!) |
| Mushrooms | Relatively high protein, nutrient-dense |
Herbal support can take different forms based on individual circumstance. Relevant herbs may have direct hypoglycemic effects or help combat insulin resistance, support the pancreas and digestive system (which can help regulate blood sugar in at least some cases*), or support other body systems strained by diabetes.
When assessing candidate herbs for direct intervention, we of course seek references to diabetes, but more commonly found are references to pancreatic enzymes or simply general use as bitter tonics. Often these herbs (or their chemical constituents) can then be found in research directly relating to diabetes (via PubMed, LibGen, etc.), or in articles focusing on enzymes that fit into our understanding of metabolic needs.
I have the most personal experience with goldenseal and its constituent chemical berberine (which is also produced by plants in other bioregions). Goldenseal is used in Indigenous medical traditions, settler folk medicine, and various historical iterations of academic western medicine as a tonic bitter that is supportive to the pancreas,14,15,16 and scientific inquiry suggests that berberine is hypoglycemic, supports insulin production, and reduces insulin resistance, though it also points out that berberine in its pure form is toxic and poorly absorbed.17,18 However, herbalists generally consider goldenseal to be quite safe. Medical herbalist Dr. Richard Whelan suggests goldenseal should not be used while pregnant or breastfeeding, is not for children, and to proceed with blood pressure monitoring in people with hypertension.19 I’ve found 1:2 weight:volume20 fresh goldenseal root tincture made with 75% ABV ethyl alcohol at normal tonic doses to acutely relieve or apparently prevent symptoms associated with hyperglycemia21 in myself on several occasions; though, I have yet to find an opportunity to test this with a glucometer.
Goldenseal is also notable as a slow-growing woodland plant in need of protective attention. Practicing mutual aid with this plant where bio-regionally appropriate may be necessary to both of our continued survival.
Indirect or holistic intervention is best drawn from a wider herbal knowledge base and tailored to individuals in context. The following table contains plants we have used or heard of being useful in managing diabetes directly or managing secondary complications. As a starting point, I recommend looking them up in some of the references provided below and/or using Google Scholar in conjunction with SciHub or Anna’s Archive to seek scientific articles about these plants.
Note: Medicinal benefits of various plants sometimes vary at the species level of western scientific taxonomy, while others are used interchangeably at the genus or even family level. Investigation into herbal references and careful experimentation with plants closely related to these native to your bioregion may yield useful results!
| Category | Specific plants | Comments |
| Antidiabetic/hypoglycemic | Goldenseal (Hydrastis canadensis), Devil’s club (Olopanax horridus), insulin plant (Chamaecostus cuspidatus), Cyperus rotundus, fringetree (Chionanthus virginicus) | Other sources of berberine such as Oregon grape (Berberis aquifolium) may also be useful. |
| Anthocyanin (red-blue pigment) cardiovascular tonics | Blueberries, tart cherries (Prunus cerasus), hawthorn berries (Crataegus spp.), hibiscus, rooibos (Aspalathus linearis) | Most red-purple foods contain anythocyanins. |
| Connective tissue-supportive mucilages | Solomon’s seal (Polygonatum spp.) and Solomon’s plume (Maianthemum spp.), mullein root (Verbascum thapsus) | Can support some cardiovascular tissues and joint issues common as secondary diabetes complications. |
| Indicated for pancreatitis | Juniper (Juniperus communis), rose gentian (Sabatia angularis),22 wormwood (Artemisia absinthium) | Especially notable in type 3c diabetes.* Possibly helpful for people at risk for diabetes through pancreatic strain and/or preventing the progression of diabetes. |
| Misc. digestive bitters | Dandelion, burdock (Arctium lappa), vervain (Verbena spp.) | Can support nutrient absorption and effective digestion; especially notable in type 3c diabetes. |
There is still a lot of work to be done and much more to figure out. If you are curious about joining autonomous medical efforts, please do. Those of us engaged in this process—from herbalists to biohackers to DIY pharmacists—are neither know-nothing bathtub drug peddlers, nor a far-off force of qualified professionals working behind the scenes to save everybody in the future. We are overwhelmingly just very desperate people trying very hard. We need more hands and minds.
SKILL UP!
Some resources for beginner herbalists:
An Anarchist Free Herbal: Beginners guide to autonomous medicine 3rd edition, (zine—it’ll come up on google)
The Herbal Medicine Maker’s Handbook by James Green
A Cree Healer and His Medicine Bundle by David Young, Robert Rodgers and Russell Willier
The Earthwise Herbal: A Complete Guide to New World Medicinal Plants by Matthew Wood
Online resources: rjwhelan.co.nz and henriettes-herb.com and phytochem.nal.usda.gov
Psst! These books are free on Library Genesis, Anna’s Archive, or the Internet Archive.
- Bernardo M et al. Real-World Data on the Adverse Metabolic Effects of Second-Generation Antipsychotics and Their Potential Determinants in Adult Patients: A Systematic Review of Population-Based Studies. Adv Ther. 2021 doi: 10.1007/s12325-021-01689-8 ↩︎
- Recommending weight loss to pre/diabetic people is horrific negligence. There is no known safe, effective method of long term weight loss; nor any evidence it would be beneficial to pre/diabetes. What we do know is that weight cycling can exacerbate metabolic problems and is extremely damaging to the cardiovascular system (possibly increasing the risk or severity of secondary complications). This is one example of how extant IWM approaches leave much to be desired even when they are accessible. ↩︎
- https://www.ellynsatterinstitute.org/family-meals-focus/11-update-stop-being-hysterical-about-obesity/ ↩︎
- E.g. type 1 diabetes or some cases of type 3c diabetes ↩︎
- Originally derived from goat’s rue (Galega officinalis) ↩︎
- If you’re interested in these efforts, biohacking spaces sometimes offer training to non-degreed prospective members. ↩︎
- https://www.awesomefoundation.org/en/projects/117138-the-open-plant-community-biology-project ↩︎
- Those interested in learning more might want to start by looking into historical insulin production. At time of writing, Wikipedia provides a good introduction. Since Wikipedia articles are subject to change, I recommend using the Wayback Machine to view an archived snapshot: http://web.archive.org/web/20241004093557/https://en.wikipedia.org/wiki/Insulin#History_of_study ↩︎
- Lower insulin demand may also improve the viability of community-based insulin production. ↩︎
- Nuttall FQ, Gannon MC. Dietary protein and the blood glucose concentration. Diabetes. 2013. doi: 10.2337/db12-1829. ↩︎
- Gatti E et al. Differential effect of unsaturated oils and butter on blood glucose and insulin response to carbohydrate in normal volunteers. Eur J Clin Nutr. 1992 PMID: 1559521. Note: Study is of poor quality but seems anecdotally verified by our experiences. ↩︎
- Wolpert HA et al. Dietary fat acutely increases glucose concentrations and insulin requirements in patients with type 1 diabetes. Diabetes Care. 2013 doi: 10.2337/dc12-0092 ↩︎
- See notes 2 and 3. ↩︎
- Bolyard, Judith. Medicinal Plants and Home Remedies of Appalachia. 1981. ↩︎
- Wood, Matthew. The Earthwise Herbal: A complete guide to new world medicinal plants. 2009. ↩︎
- Theory of disease varies between medical traditions while use cases remain relatively consistent, originating with Indigenous traditions and later picked up by settlers with various rewriting of how these medicinal actions are conceptualized. ↩︎
- Yin J, Xing H, Ye J. Efficacy of berberine in patients with type 2 diabetes mellitus. Metabolism. 2008. doi: 10.1016/j.metabol.2008.01.013. ↩︎
- Utami AR, Maksum IP, Deawati Y. Berberine and Its Study as an Antidiabetic Compound. Biology (Basel). doi: 10.3390/biology12070973. ↩︎
- https://rjwhelan.co.nz/herbs%20A-Z/goldenseal.html ↩︎
- A standard notation for strength of tinctures; see The Herbal Medicine Maker’s Handbook (Chapter 12, page 246), mentioned below. ↩︎
- Fatigue, extreme thirst, and peripheral neuropathy after multiple days of almost exclusively eating simple carbs ↩︎
- Several plants known commonly as “gentian” are used for this purpose despite varying genetic relation. Look up your local “gentian”-named plants by scientific name in herbal references to see if they are used medicinally or if they are closely related to a known medicinal species. ↩︎
